Spotlight: Songkhla Province
Scaling up HIV-related stigma reduction activities at
the subnational level
Background
Songkhla Province is located approximately 750 km south of Bangkok.

(Figure 1). The province has a population of 1.4 million spanning 16 districts that is served by 17 hospitals. These hospitals provide care to nearly 8,000 people living with HIV (PLWH) in the province.
As part of the Division of AIDS Services’ efforts to eliminate HIV-related
stigma and discrimination (S&D) in healthcare settings throughout Thailand, in 2017 Songkhla Province was selected to implement S&D-reduction activities in two of its community hospitals—Chana and Satingpra. Applying lessons learned from this initial work, the province developed a coordinated strategy to scale up S&D-reduction activities in additional hospitals throughout the province, including its two large general hospitals.
An Evidenced-Informed Approach to Scale Up
Organization of S&D-Reduction Activities
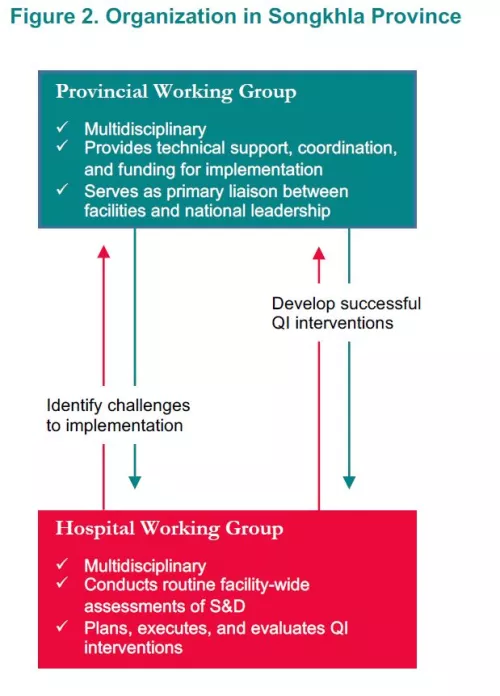
To ensure accountability and optimal monitoring of the initiative, the Songkhla Provincial Public Health Office developed a layered approach to organization of activities, spanning province- and hospital-level leadership (Figure 2). At the provincial level, an S&D working group was convened with representatives from the Provincial Health Office, the Departments of Education, Justice, Social Welfare and Labor Protection, together with local PLWH advocacy organizations. The primary functions of this working group are to provide on-site technical support, facilitate exchange among implementing hospitals, and lead monitoring and evaluation activities. At the hospital level, activities are led by an S&D working group comprising administrative leadership, clinicians, and PLWH. With support from the provincial working group, the hospital S&D working groups collected baseline and follow-up performance data, convene hospital-wide training, and devise and implement QI interventions.
As part of initial planning, the provincial working group developed a plan for scale up. Lessons learned from initial implementation in the first wave of hospitals (Chana and Satingpra) were continuously harvested to inform subsequent waves of implementation. Through this “learning-by-doing” approach, the Province choose to independently expand implementation beyond the initial pilot hospitals to implement S&D-reduction activities in nine additional provincial hospitals over the span of three years.
Initial Results of HCW Surveys
As part of the first wave of implementation, teams from Chana and Satingpra carried out a baseline assessment of S&D among their healthcare workers (HCWs) and identified potential interventions using root cause analysis. As part of this initial assessment, 308 HCWs between the two hospitals were surveyed. Initial results revealed high levels of worry related to occupational HIV exposure, with 47% of HCWs expressing worries about drawing blood from a PLWH 49% expressing worries about dressing the wounds of PLWH, and 43% agreeing that they avoid touching the clothing or belongings of HIVpositive patients. In addition, 38% reported wearing double gloves when caring for PLWH, 13% have witnessed colleagues unwilling to care for PLWH, and 11% have witnessed colleagues providing poorer quality of care to PLWH relative to HIV-negative patients.
Interventions
Using initial results collected at Chana and Satingpra Hospitals, strategies were identified and harvested for scale up. These strategies included delivery of national S&D-reduction curriculum for all HCWs, elimination of HIV-specific labeling and coding procedures for charting and hospital beds, bolstering and reinforcing infection control curricula, integration of S&D reduction activities with existing QI and Hospital Accreditation activities, and convening of case conferences on stigma reduction.
Results
Following implementation, surveys of HCWs (n=348) were repeated. Results showed improvements across multiple measures, including decreases in worries surrounding occupational HIV transmission (through patients’ clothing and dressing wounds), and use of double gloves when caring for PLWH. Notably, several indicators remained largely unchanged; in particular, there was no change in the proportion of HCWs who noticed colleagues unwilling to care for PLWH, and limited change in the proportion of HCWs reporting worry about drawing blood from PLWH.

Lessons Learned
Through its evidence-informed approach to scale up, the work of Songkhla Provincial Public Health Office offers important lessons on how sub-national health authorities can effectively organize, coordinate, and scale S&D reduction activities:
- Designating a central leadership team. Strong leadership is a key enabler of quality improvement. By organizing a central leadership team to oversee S&D-reduction activities, the Province was able to ensure an efficient, coordinated use of resources, create a culture inducive to change, and rally support for participation in S&D-reduction activities.
- Planning for scale up from the start. As a complex intervention, S&D reduction can be difficult to scale up in a health system. In its use of a “learning-by-doing” approach, Songkhla Province was able to gather, synthesize, and apply lessons learned from initial implementation to inform the effective spread of activities to additional facilities. By using this stepwise approach, the provincial team not only identified strategies to address common barriers to implementation, but also championed, and shared, the initial successes in Chana and Satingpra Hospitals to gather buy in for continued scale up.
- Developing a multidisciplinary approach to S&D-reduction activities. At all levels of organization, S&D-reduction activities in Songkhla Province were supported by a multidisciplinary team approach involving stakeholders from PLWH advocacy organizations, participating health facilities, and other provincial departments. As HIV-related S&D is complex and may be deeply rooted in attitudes, behaviors, policies, and law, a multidisciplinary team approach can be highly effective in tackling S&D across these many fronts through shared expertise, accountability, and resources.
Acknowledgements
In its production of this Spotlight, UCSF-HEALTHQUAL acknowledges Dr. Charoensuk Chanovunna of the Songkhla Provincial Public Health Office and the Division of AIDS Services for their contributions and careful review, and Chiang Mai University for its ongoing technical assistance. The Southeast Asia Stigma Reduction QI Learning Network is supported financially by Gilead Sciences, Inc., and ViiV Healthcare. The contents are the responsibility of UCSF-HEALTHQUAL and do not necessarily reflect the views of Gilead Sciences, Inc., or ViiV Healthcare.